Biochemical Profile
Classification: Water-soluble vitamin (B-complex family)
Chemical Structure/Properties: Folate is a term for a family of related compounds based on a pteroylglutamic acid structure, composed of a pteridine ring, para-aminobenzoic acid (PABA), and one or more glutamate residues. In nature (food folate), it typically exists in a reduced, polyglutamated form. The synthetic, oxidized, monoglutamate form used in supplements and food fortification is termed folic acid. The primary biologically active form in the body is tetrahydrofolate (THF) and its derivatives, such as 5-methyltetrahydrofolate (5-MTHF).
Metabolic Function & Mechanism
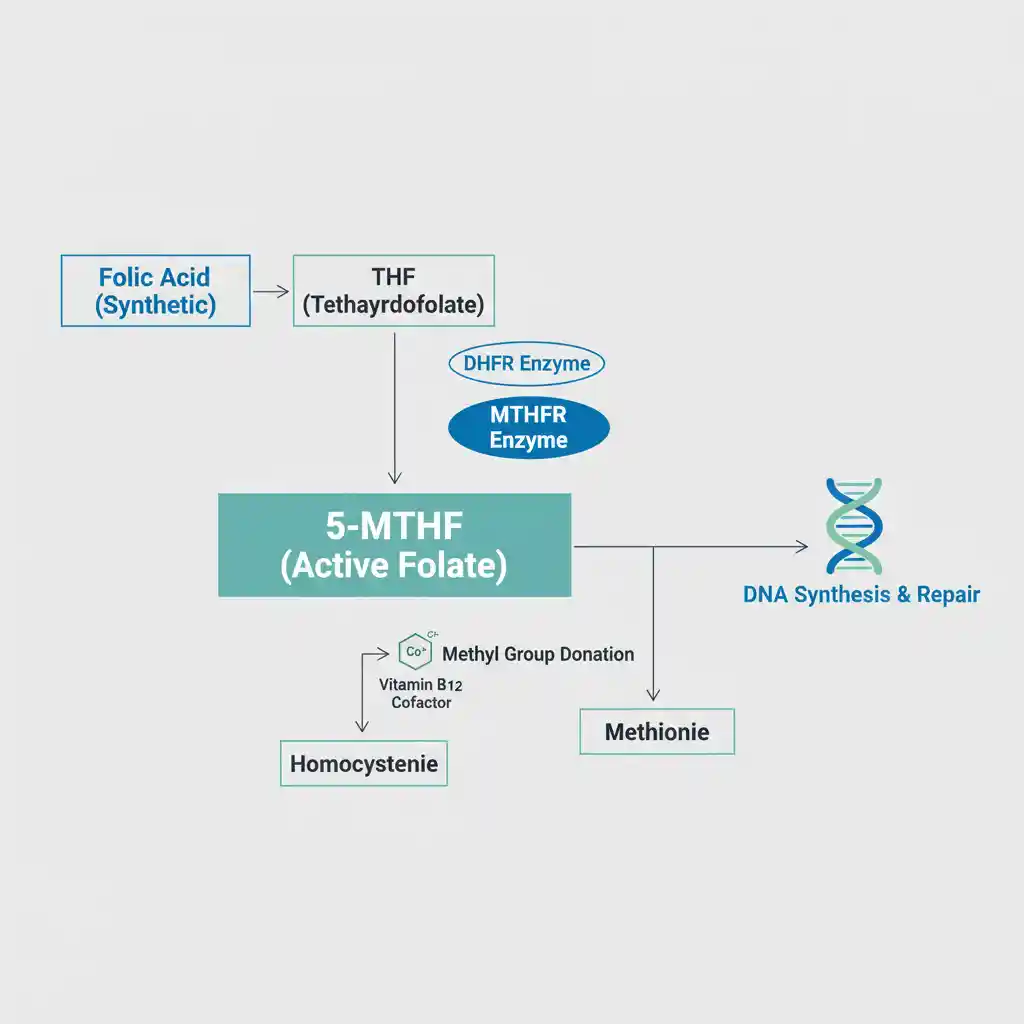
Folate’s central role in metabolism is as a coenzyme in the transfer of single-carbon units (e.g., methyl, formyl groups). This process, known as one-carbon metabolism, is fundamental for DNA synthesis and repair, as well as methylation reactions.
Absorption of dietary polyglutamated folate requires hydrolysis to the monoglutamate form in the jejunum. Synthetic folic acid, being a monoglutamate, is more readily absorbed. Once in the cell, folic acid must be reduced to THF by the enzyme dihydrofolate reductase (DHFR). THF is then converted into various coenzyme forms. A critical step is the irreversible conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate (5-MTHF) by the enzyme methylenetetrahydrofolate reductase (MTHFR). 5-MTHF then donates its methyl group to convert homocysteine to methionine, a reaction catalyzed by methionine synthase, which requires Vitamin B12 as a cofactor.
Medical Nutrition Therapy (MNT) Applications
The clinical applications of folate are directly linked to its role in cell division and methylation.
- Prevention of Neural Tube Defects (NTDs): Adequate folate status before and during early pregnancy is critical for neural tube closure in the fetus. MNT involves recommending folic acid supplementation for all women of childbearing potential, a cornerstone of public health policy.
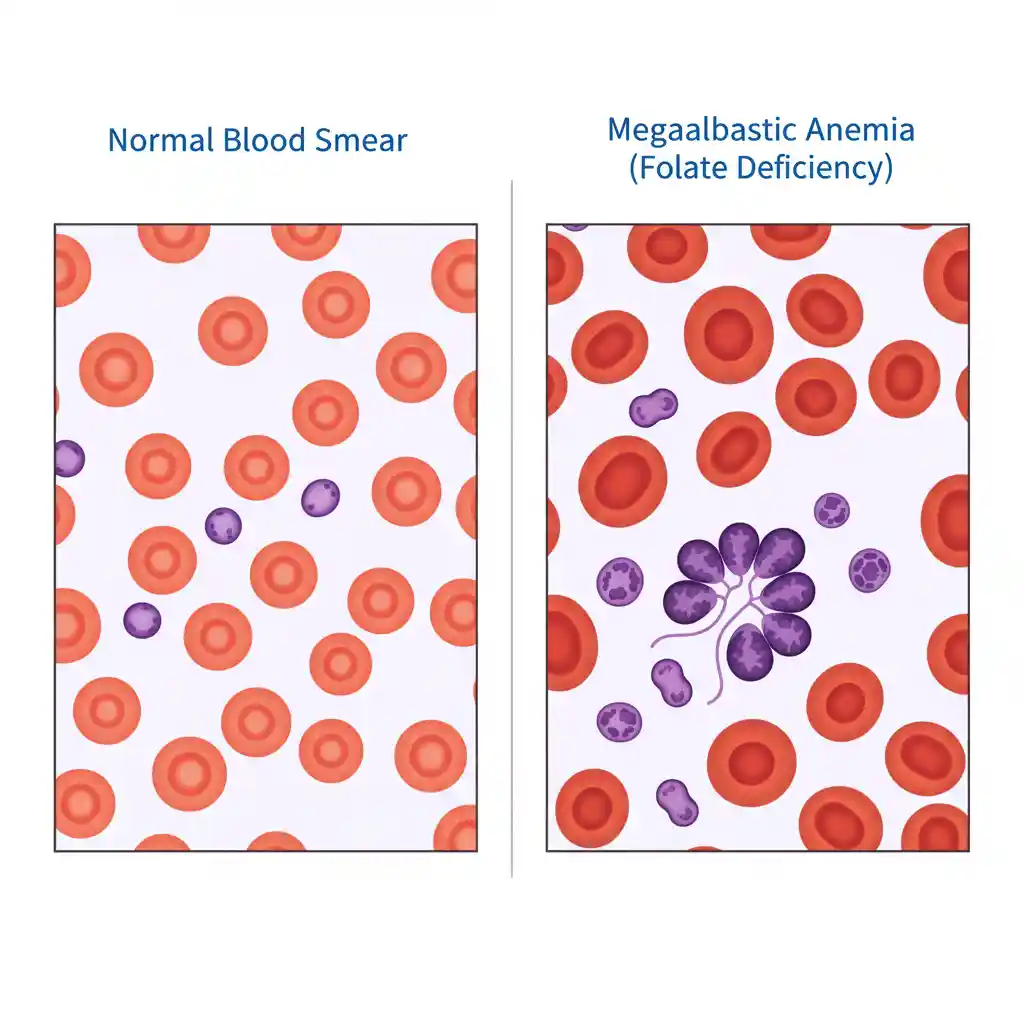
- Megaloblastic Anemia: Folate deficiency impairs DNA synthesis, leading to the production of large, immature red blood cells (megaloblasts) and resulting in anemia. MNT involves high-dose folate supplementation to restore normal erythropoiesis.
- Hyperhomocysteinemia Management: Elevated plasma homocysteine is an independent risk factor for cardiovascular disease. As folate is essential for homocysteine metabolism, MNT with folate (often in combination with vitamins B6 and B12) is used to lower homocysteine levels.
- MTHFR Gene Variants: Individuals with certain polymorphisms in the MTHFR gene may exhibit reduced enzyme activity, leading to less efficient conversion of folate to its active 5-MTHF form. In these cases, MNT may involve supplementation with L-5-MTHF directly to bypass this metabolic step.
Dietary Sources & Bioavailability
The bioavailability of folate varies significantly depending on its chemical form. Food folate is estimated to be about 50% as bioavailable as synthetic folic acid due to its polyglutamate structure and instability during processing.
| Source | Form of Folate | Estimated Bioavailability |
|---|---|---|
| Dark Leafy Greens (e.g., Spinach) | Natural Folate (Polyglutamate) | ~50% (Heat-labile) |
| Legumes (e.g., Lentils, Chickpeas) | Natural Folate (Polyglutamate) | ~50% |
| Fortified Breads & Cereals | Folic Acid (Synthetic Monoglutamate) | ~85% (consumed with food) |
| Folic Acid Supplement (fasting) | Folic Acid (Synthetic Monoglutamate) | ~100% |
| L-5-MTHF Supplement | Active Folate (5-MTHF) | High (Bypasses MTHFR conversion) |
Safety & Interactions
The Institute of Medicine has established a Tolerable Upper Intake Level (UL) for synthetic folic acid at 1,000 mcg/day for adults. The primary safety concern with high doses of folic acid is its potential to mask the hematological signs of a Vitamin B12 deficiency. By correcting the megaloblastic anemia, it can delay diagnosis of the B12 deficiency, allowing potentially irreversible neurological damage to progress.
- Drug-Nutrient Interactions:
- Methotrexate: This chemotherapy and anti-inflammatory drug is a folate antagonist that inhibits the DHFR enzyme. High-dose folic acid supplementation can interfere with its therapeutic action.
- Anticonvulsants: Drugs like phenytoin, carbamazepine, and phenobarbital can impair folate absorption and increase its catabolism.
- Sulfasalazine: Used for inflammatory bowel disease (IBD), it can inhibit the intestinal absorption of folate.